Black History Month creates a moment when we can step back and reflect together, as well as individually, on the immense contribution of Black, Asian and minority ethnic communities whose rich history, culture, and experiences, have shaped Brent and beyond.
The NW London Joint Health Scrutiny Committee comprises 8 NW London boroughs. As Chair, I know we simply could not function without the dedication, the skills, and above all, the compassion that thousands of people from our diverse communities contribute to the NHS, day in and day out.
The difference this makes to all our lives, is immeasurable. Black History Month affords us an opportunity to acknowledge and thank them for the important work they do: their continuing contribution to the care, the culture, the shaping, and well-being of Brent.
The colour of someone’s skin should not determine how they are perceived, considered, and treated – positively or negatively – but the impact of the pandemic has highlighted many disturbing features of inequality in our communities. Many of these problems are not new. They have existed for far too long.
Black, Asian and minority ethnic communities are more likely to be affected by life-changing diseases like diabetes, prostate cancer, and sickle cell than people from other backgrounds. Living in less-affluent areas, they are more greatly affected by poor housing as well as poor air quality from the busy urban roads that run through their neighbourhoods. There is a big gap in life expectancy between richer and poorer areas irrespective of race, but these communities are disproportionately affected.
To tackle these inequalities, the North West London Integrated Care System is launching a joint initiative between the local NHS and NW London boroughs, which will seek to build real understanding of what matters to our residents, how we can work with them to remove barriers to health equality to deliver healthier neighbourhoods and better outcomes.
This initiative is the first tangible benefit I have seen emerge from the new Integrated Care System, which has health services and local authorities coming together to address many of the challenges that impact our well-being. That is, health and care services, employment, education, housing, and the environment we live in.
We might perhaps reflect for a moment on the work of the great poet, James Berry OBE, who never avoided the difficult issues of injustice in history, or in the present, but always sought for mutual understanding. His poem, “Benediction,” stresses the need for us truly to hear one another, and truly to see, and through so doing, to understand. He said:
Thanks to the ear that someone may hear
Thanks to seeing
that someone may see
Thanks to feeling
that someone may feel
Thanks to touch
that one may be touched…
Black History Month is a reminder to us to truly hear and see one another, to celebrate our heroes and tell the stories that, for so long, have been hidden or forgotten. It is also a reminder that the evils of the past have resonance today, reflected in the impact of poverty and institutional racism that many in our communities experience as part of their daily lives. Ultimately, it is an opportunity to continue to learn, understand and come together to pull down these barriers and build healthier and fairer neighbourhoods.
Cllr Ketan Sheth is Chair of Brent Council’s Community and Wellbeing Scrutiny Committee
Mortality rates during the pandemic laid bare the health inequalities that exist across the country. Behind these figures lie human stories and grieving families that should remind us of the urgency and importance of understanding and addressing these inequalities.
In Brent, an ethnically diverse North West London borough, we recently set out to do just that.
Systems thinking
We know that Brent residents, who are from ethnic minority communities, disabled, or who are in poverty, experience significant health inequalities; but what does that look like in practice? How are our healthcare systems contributing to and/or compounding inequality? And what can be done to resolve this challenge?
Usually, GPs are the first point of call when someone is not feeling quite right. They ought to help everyone to access timely and safe healthcare. Therefore, reviewing access to GP services is critical and we decided to focus a dedicated scrutiny task group for eight months to report.
By giving ourselves time to understand this complex area in detail, we developed a deep comprehension of the landscape we were going to scrutinise. Patient voices are at the heart of our work, and we worked closely with Brent Healthwatch to ensure those from communities that have been under-represented in these conversations in the past, as well as those experiencing the worst health outcomes, were able to articulate and share their experiences.
Also, the task group held a number of evidence sessions over the course of six months, which were attended by stakeholders across Brent’s health economy. This included council officers, local commissioners and service providers.
All of this enabled the team to make a number of practical recommendations to Brent Council and NHS partners.
Our work focused on three pivotal areas: Demand, Access and Barriers
With the dynamics of our healthcare and well-being landscape changing locally as well as nationally, it is more vital than ever to ensure all our residents have equality of access and consumption of healthcare services.
We found repeatedly that some groups of patients experience significant, and unnecessary, barriers, specifically:
• Patients of low-income
• Patients with a disability
• Older patients
• Patients whose first language is not English
• Children and young people
• Refugees and asylum seekers
• Patients who cannot access digital technology
Knowing this, GP services must seek to reduce and resolve the barriers experienced by patients, with a focus on deprivation, ethnicity, disability, and other protected characteristics as described in the Equalities Act 2010, if we are to execute our duties under the Act.
We recognise that rising demand, changing patient expectations and workforce retention issues continue to place pressures on primary care. Therefore, it is essential that the NHS continues to plan for this and uses the expertise of healthcare professionals across the system.
The digital transformation to healthcare, brought about by the pandemic, although helpful to some, introduced additional barriers for other people and communities.
In acknowledging the varying levels of ease in which patients access GP service, we strongly believe an access and treatment standard ought to be developed. This will ensure that Brent residents experience consistent and high levels of service: whether their requests are routine or urgent, focused on physical or mental wellness; or made via the telephone, online or in-person.
Our work has been conducted in the spirit of cooperation and partnership, and particularly, we look forward to continuing our dialogue and work with our partners across Brent’s health economy to evolve our shared vision of GP access across Brent.
Cllr Ketan Sheth is Chair of Brent Council’s Community and Wellbeing Scrutiny Committee
Fresh from winning the Grand Jury Prize at the Banff Rockie Awards on Monday, Channel Four’s drama Help was yesterday nominated for Best Drama in the Edinburgh TV awards, with its lead actor Jodie Cromer also nominated for Best Actor. The drama was one of the most watched on the channel, bringing to millions of viewers the plight of care homes and their residents during the pandemic. Whilst the Help storyline is fictional, it is based on hard and devastating facts.
In my view, Help could be criticised for its farfetched ending and sometimes unsympathetic rendering of the care home manager, however its characterisation of care home staff and residents is both caring and revealing. Clearly emotionally affected researching the programme, writer Jack Thorn said: “hearing the stories of those at the frontline, having people break down in tears on zoom in front of us has been incredibly moving and galling”.
My two favourite parts of the programme (no spoilers) are the endless recorded message of a hopelessly over-run “NHS 111” call centre in the background for several minutes, and Jodie Cromer’s wrenching speech to camera (1:34 on the video) demanding “…underlying health conditions, eh? When did all lives stop being worth the same?” The programme ends highlighting some stunning research findings: 40% of Covid deaths in the early pandemic (from March to June 2020) were in care homes; the average wage of a care home worker is £8.50 per hour; whilst government provided 80% of PPE needs for the NHS, it only met 10% of adult social care’s needs.
This last claim is based on the National Audit Office analysis published in November 2020, which found that the adult social care sector received approximately 331 million items of PPE from central government between March and July (10% of their estimated need) whereas NHS trusts received 1,900 million items sent to NHS trusts (80% of estimated need). Whilst both fell significantly short of what was required, there is an apparent imbalance here. Data collected by the Care Quality Commission (CQC) showed that, throughout April and May 2020, more than a fifth of domiciliary care providers had no more than a week’s supply of PPE.
This situation was well known to the Secretary of State, not least because the LGA and the Association of Directors of Adult Social Services wrote stating “we continue to receive daily reports from colleagues that essential supplies are not getting through to the social care front-line. Furthermore, national reporting that equipment has been delivered to providers on the CQC-registered list does not tally with colleagues’ experience on the ground”. Nevertheless, in a scene included in Help, during a Downing Street press conference on 15 May, 2020, Mr Hancock said: “right from the start, it’s been clear that this horrible virus affects older people most. So right from the start, we’ve tried to throw a protective ring around our care homes”, repeating in the House of Commons on 18 May that “we absolutely did throw a protective ring around social care”.
Understanding the human costs of these central government failures is difficult, with the effects on staff, residents and their family impossible to measure objectively. Help does a good job in illustrating some of the pressures on care staff and the pain of relatives unable to visit dying residents, made all the more poignant now that we know some of the behaviour during the pandemic of senior central government actors such as Hancock’s affair and Johnson’s multiple parties forensically examined in Sue Gray’s recent report.
Perhaps the most basic measure is in human lives. Last year researchers used the national death registry of all adult (aged ≥18 years) deaths in England and Wales between January 1, 2014, and June 30, 2020 to compare daily deaths during the COVID-19 pandemic against the expected daily deaths. They estimated that during the early pandemic, about 26,000 excess deaths (almost half of the total excess deaths) occurred in care homes and hospices. This is likely to be an underestimate since early in the pandemic, testing of suspected cases was available only in the hospital, whereas routine testing of staff and residents in care homes was not implemented until May 2020.
The latest ONS statistics, issued in February 2022, suggest that since the beginning of the coronavirus (COVID-19) pandemic, there have been over 274,000 deaths of care home residents (wherever the death occurred) registered in England and Wales; of these, 45,632 involved COVID-19 accounting for 17% of all deaths of care home residents.
Intriguingly, The Lancet reported in March that “COVID-19 has had a disproportionate impact on the mortality of care home residents in England compared to older residents of private homes, but only in the first wave. This may be explained by a degree of acquired immunity, improved protective measures or changes in the underlying frailty of the populations.” Meanwhile, last month the Care Quality Commission finally published data on deaths in each care home during the first year of the pandemic (April 2020 to March 2021).
Whatever the precise figures, it’s clear that adult social care residents and staff were badly let down by central government, far from the Secretary of State’s “protective ring” narrative. This despite the best efforts of care managers, local commissioners and councils discussed in Luke Bradbury’s blog here last week. Help does a fantastic job of showing the impact of these critical central failures – and recognising the incredible work care staff did in such difficult circumstances with so little financial reward.
The publication last month of the Institute for Government’s report on the impact of cuts in local services during the decade of austerity has revealed to the public what has been obvious in the sector for years – austerity was hugely unfair and hit the poorest hardest.
Neighbourhood services under strain is written in IfG’s usual forensic style, and its conclusion is all the more brutal because of it: the most deprived areas received the biggest grant cuts, resulting in bigger reductions in local services such as libraries and recycling. Central government grants were cut more in deprived areas because of the way cuts to grant funding were distributed ignoring councils’ different degree of dependency on this income source. Because of the central cuts and pressures such as the increasing demand for social services, councils have been forced to cut preventative and universal services like children’s centres and housing programmes to help vulnerable people to live independently.
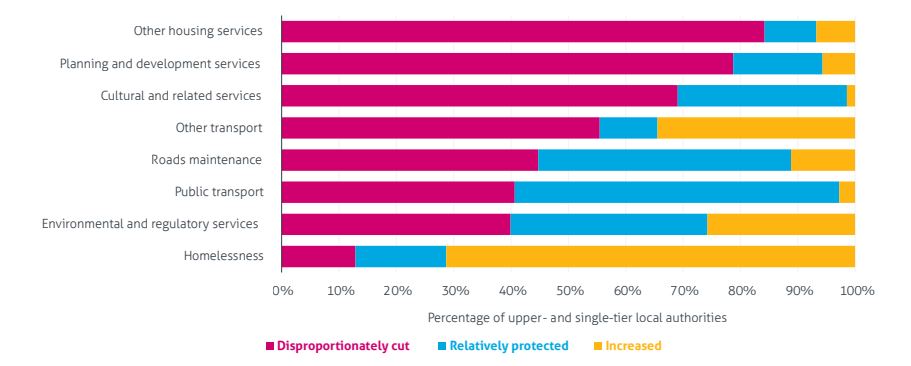
The report’s detailed analysis of changes in spending reported to DHCLG concludes that most councils chose to protect similar services. ‘Relatively protected’ services included environment and regulatory services, homelessness and public transport. At the other extreme, most councils applied higher than average spending cuts in housing, cultural, and planning services (figure 1 below). This mirrors earlier analysis by the National Audit Office (which also highlighted the protection of social care services).
Figure 1: Local authorities that disproportionately cut, relatively protected, or increased neighbourhood services spending between 2009/10 and 2019/20, by category
Source: Institute for Government analysis of DLUHC, Local authority revenue expenditure and financing in England: individual local authority data – revenue outturn 2009/10 and 2019/20.
The IfG report hints at the innovative ways different councils responded to these pressures, from contract renegotiation and the use of new technology, to service redesign and rationalisation. For a more detailed exploration of this, I recommend Alison Gardner’s excellent thesis on how local councils responded to austerity – including strategic asset management, shared services, commercialisation, co-production and demand management. Whatever methods were used, however, it’s clear that by the second half of the decade of austerity the cuts were no longer into ‘fat’ but into ‘flesh’.
These new findings add to a growing library of research on the effects of the UK government choice to pursue austerity policies, including a BMJ study in October 2021 which suggested that the constraints on health and social care spend during this period of ‘austerity’ have been associated with 57,550 more deaths than would have been expected had the growth in spend followed trends before 2010. Considering cuts to local government funding specifically, a July 2021 study in The Lancet estimated that cuts in funding were associated with an increase in the gap in life expectancy between the most and least deprived quintiles by 3% for men and 4% for women between 2013 and 2017. Overall reductions in local government funding during this period were associated with an additional 9,600 deaths in people younger than 75 years in England. Well before the pandemic, the UK was seeing a rapid slowdown in life expectancy gains in the 2010s and, although a number of other high income countries also saw such slowdowns, of large populations only the USA experienced a more severe slowdown/reversal and the magnitude of the slowdown in the UK was more severe than other large European populations.
Perhaps the most damning finding of the IfG report is that central government lacks the information to know what the impact of its spending cuts are on local services. This echoes the assessment of the Nuffield Trust and Health Foundation back in 2014 which warned government was making decisions with ‘no comprehensive way to quantify the impact that social care cuts are having on their health and wellbeing’ and were therefore effectively ‘flying blind’. Having abolished the Audit Commission in 2010, the government was left with no comparable performance statistics for two-thirds of local services. Some may believe that this was quite convenient, given what we are now learning about the effects of that government’s spending policies.
Most of us can remember as teenagers those exciting moments of independence, of achieving the landmarks of adulthood; perhaps learning to drive; our first relationship; our first job. These landmarks all signify moments of increasing maturity, of independence, but each of these landmarks remind us that there is no one moment of independence. We don’t flip a switch to become a grown-up – one day a child, one day an adult. Maturity is a gradual process, a high wire that we walk where most of us benefit from a safety net of parents, family, friends.
For our most vulnerable children and young people too, there isn’t a switch and sadly too often they don’t have the safety net they need. There is now much more emphasis on the transitional period so that services extend from aged 16 to around 25. There should not be abrupt changes to a service just because someone reaches the age of 18, with its attendant risk of falling between the gap where services don’t always join up!
In recent years, safeguarding children and adults has become increasingly complex, with risks such as sexual exploitation, gang and group offending and violent crime challenging the children’s and adults’ safeguarding workforce to identify opportunities for innovation. The notion of transitional safeguarding is an emerging one, not currently widely applied in policy or practice. Its implementation requires changes in policy and practice and across systems involving all agencies.
However, some local authority areas, like Brent, are already innovating and creating opportunities for more flexible and bespoke support, and providing valuable experiences for young people at a key point in their lives. This makes sense in most circumstances, but keeping vulnerable young people safe as they transition from adolescence to adulthood challenges us all to remember that becoming an adult is a process of transition, of many moments.
Transitional safeguarding is an emerging area of practice where we challenge ourselves in public service to make sure we keep that safety net in place; that we help keep safe and promote the well-being of our young people when they need it most, regardless of the artificial barriers of age, and including during those important times of transition to adulthood.
Supporting young people’s safety and well-being during the transition to adulthood is not only morally and ethically important, but it is also important for the future health of society and future generations. Young people may experience a range of risks and harms which may require a distinct multi-agency safeguarding response, and safeguarding support should not end simply because a young person reaches the age of 18. Investing in support to address harm and its impacts at this life stage can help to reduce for the need for specialist and statutory intervention and criminal justice involvement later on in life.
In Brent, my scrutiny committee recognises the importance of taking this holistic, broad view for our Brent young people. We believe we are well placed to be at the vanguard of these developments, with promising pilot work, in collaboration with partner organisations, already completed to change and enhance services; and my scrutiny committee are recommending that Brent develops a council-wide approach to transitional safeguarding by working with those young people who need us most.
And most importantly, I think that everybody has a valuable contribution to make to the transitional safeguarding agenda to help improve our practice for the better outcomes of all our most vulnerable young people; and indeed, the service is there when they need to use it.
Cllr Ketan Sheth is Brent Council’s Chair of Community and Wellbeing Scrutiny Committee
Inter-municipal collaboration, often referred to as ‘shared services,’ has gained a significant foothold in English local government over the last 10-15 years, bringing England into line with much of mainland Europe and the USA.
This model of jointly providing public services across two or more local jurisdictions, whether through a ‘joint committee’ or ‘lead authority’ model, or by joint commissioning of a private contractor, was primarily intended as an efficiency measure through which cash-strapped councils might attain new economies of scale during the ‘age of austerity.’ Limited evidence to date unfortunately suggests that councils’ large cost-saving aspirations have not tended to be been matched by achievements, though more research is needed.
Nonetheless, when councils and management consultants were preparing their ambitious shared service business cases, typically in the early 2010s, improved service quality and better resilience in the face of unexpected adversity were also named as advantages of the shared services approach, alongside efficiency. Since efficiency and resilience are often regarded as mutually incompatible (e.g., slack resources are inefficient but protective against shocks), and given that there are few if any empirical tests of the relationship between shared services and business continuity in existing literature, we set out to investigate.
Taking the first Covid-19 lockdown during the spring of 2020 as the sudden and severe ‘adversity’ against which local government resilience was tested, we compared levels of service disruption in collaborating and autonomous councils compared against pre-covid performance, controlling statistically for potential alternative explanations. Our analysis focuses on revenues and benefits departments in district councils, since a significant proportion of these (ca 30% at the onset of Covid-19) are operated collaboratively. And we focus on the administration of Housing Benefit specifically, for which robust, high-frequency (monthly and quarterly), and multi-dimensional (speed, quality and cost) performance data is available.
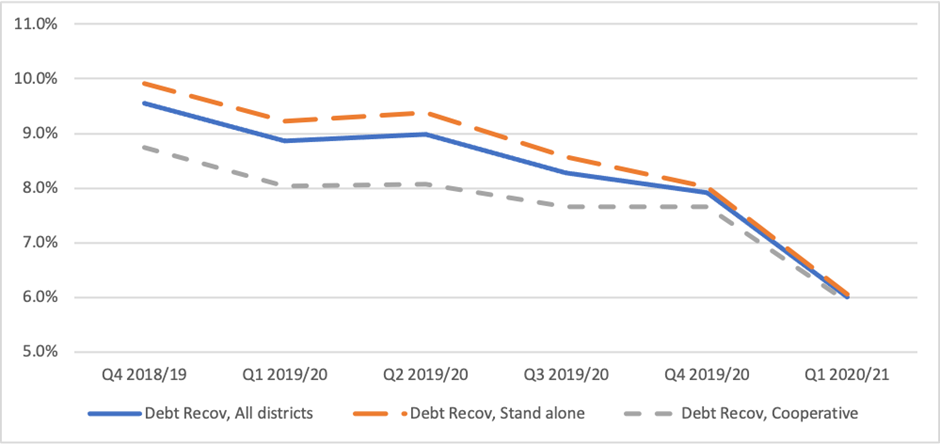
Our study found that disruption of Housing Benefit application processing speeds during lockdown was unrelated to mode of service provision. For both shared and autonomous arrangements, performance worsened slightly during lockdown, before resuming its pre-pandemic trajectory over the summer of 2020. However, collaborating councils did show less of a decline in service accuracy objectives during lockdown, measured as both the identification of new debt owing to benefit overpayments (not shown) and, particularly, the recovery of such debt from claimants (shown in the graph below). These mixed results – no effect on speed, partial protection for accuracy – proved robust to various different econometric specifications.
Average value of debt recovered from Housing Benefits claimants as percentage of total debt outstanding, comparing ‘stand alone’ and collaborative provision, Q4 2018–19 to Q1 2020–21
There are a variety of possible explanations for this pattern.
First is that the apparent resilience in debt identification and recovery is simply an artifact of the performance differential between shared and autonomous revenues and benefits departments pre-pandemic. As the graph above indicates, and contrary to business-case predictions, shared services (grey dashed line) appear to be consistently associated with less debt recovery prior to COVID, meaning that autonomous councils simply had ‘further to fall’ during the emergency, producing their appearance of reduced resilience.
Second, and more substantively, is that high-performing organizations can fall into ‘success traps’ or ‘competency traps.’ According to existing literature on organizational resilience, the low level of challenge facing high-performing organizations during ‘normal’ times can leave them complacent and ill-equipped to deal with unexpected adversity; whereas less-successful organizations are more familiar with confronting and managing adversity in their everyday operations, and thus better rehearsed for managing crises.
Third is that there genuinely is something about the shared services model – be it the increase in operating scale, the balancing of peaks and troughs in demand and resourcing across different partners, the greater experience of remote working prior to COVID, or the lock-in effects that arise when service operations are specified in contracts or service-level agreements – that enables collaborative arrangements to better withstand the challenges of service delivery during lockdown.
Finally, it is interesting to consider why the partial resilience revealed in our data is concentrated on debt identification and recovery, rather than speed – recognizing that bureaucracies often face a trade-off between speed and accuracy of decisions.
Studies of goal conflict suggest that organizations can cope with such split objectives by prioritizing those that are most valued by their largest or loudest constituency. Benefit claimants and their landlords favour speedy service, whereas central government (which funds Housing Benefit) advocates accuracy. But perhaps Whitehall overseers pursued this agenda less forcefully during the pandemic, when many distractions arose and when preservation of life and livelihoods was clearly better served by providing speedy financial support to vulnerable populations than by auditing prior applications.
Alternatively, goal conflict can also be address by sequencing – addressing one goal first, and then another. Whereas poor timeliness of benefit processing cannot be subsequently rectified (once a payment is late, it is late), poor accuracy can be corrected subsequently through greater attention to and resourcing of debt collection later in the year or in future years. The debt will still be owed, albeit the risk of debt write-off will be higher. Future research will be able to test this ‘catch-up’ hypothesis once data on debt identification and recovery during subsequent quarters of the pandemic is released.
Overall, then, in contrast to the questionable financial benefits of shared service adoption in the English context, this study has indicated that possible advantages may be gained in terms of service resilience. We have just secured a research grant to replicate and expand this research agenda into additional service areas and over a longer time frame.
Dr Thomas Elston is Association Professor of Public Administration at the Blavatnik School of Government, University of Oxford. His research focuses on the organisation of public services, and particularly on questions of performance, resilience, reform and democratic control. His work on shared services has been published in JPART,Public Administration, Public Management Review, and Public Money & Management.
Dr Germà Bel is Professor of Economics and Public Policy at the University of Barcelona. His research deals with the reform of the public sector, with a special focus on privatization, regulation, and competition. His research pays particular attention to local public services, transportation, and infrastructure. His work on shared services has been published in JPART,Public Administration,Public Management Review, Local Government Studies and Urban Affairs Review.