It’s been an exciting month in government, nationally and locally, since the General Election on 4th July. As the new Labour administration finds its feet, somewhere on Ministers’ “to do” list will be local government performance and (the department formerly known as) DLUHC’s attempts to improve this through the establishment of OFLOG, the Office for Local Government.
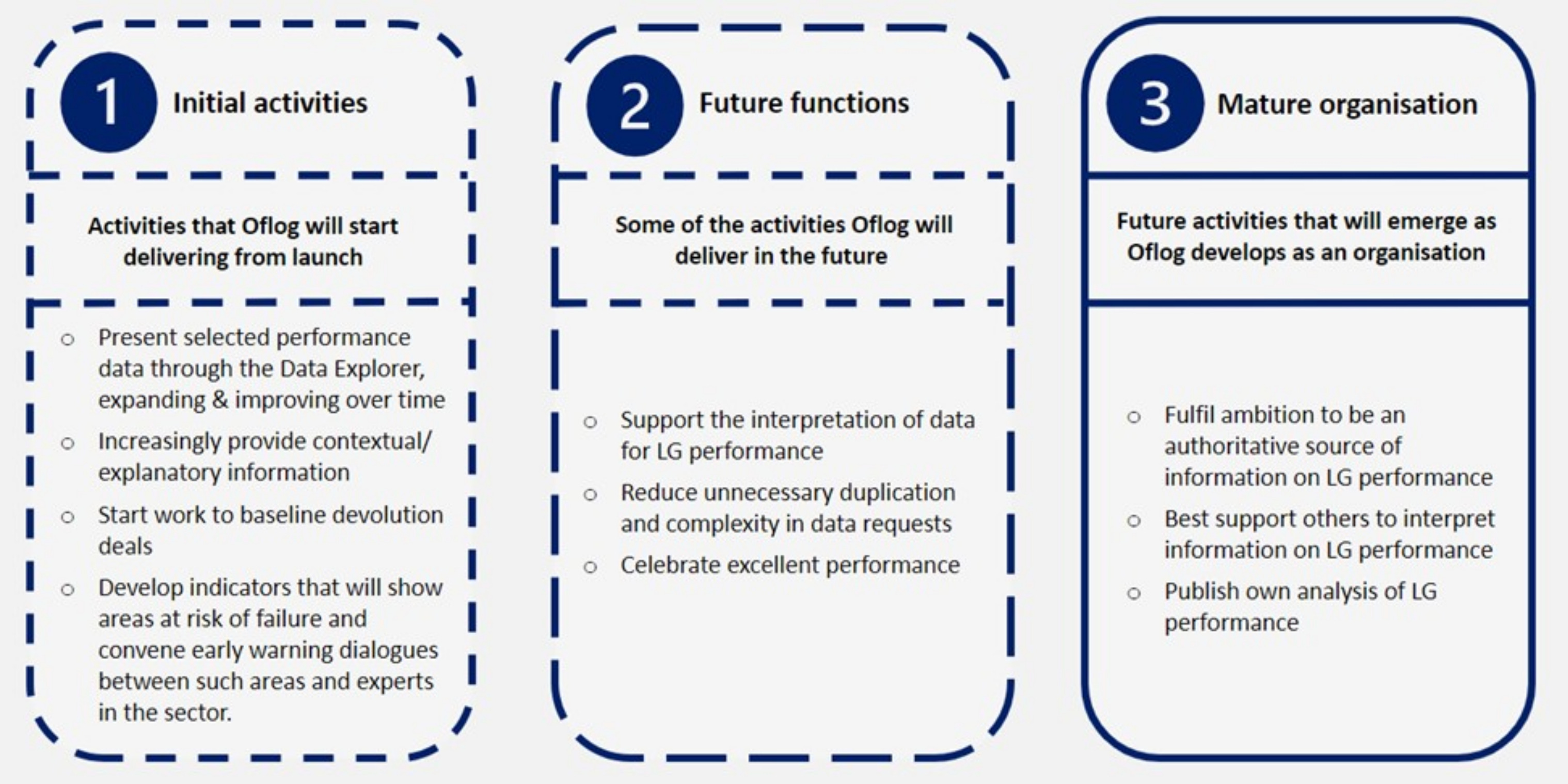
The election marked the exact anniversary of Michael Gove’s statement setting up OFLOG through the policy document, Understanding and supporting local government performance. Its remit was “to provide authoritative and accessible data and analysis about the performance of local government and support its improvement”.
Gove was at pains to stress “this is not about recreating the Audit Commission”. With that point at least, I agree. Whereas the Audit Commission was fiercely independent, often willing to criticise government policy where it was a factor in poor performance, OFLOG was established as an office of the department within the DLUHC department itself. Whereas the Audit Commission developed comprehensive performance measures which were rigorously audited to assure consistency, OFLOG picked 27 PIs and published these. Whereas the Audit Commission provided detailed national studies to inform best practice in local services, sometimes leading to wholesale systems change such as around youth justice services, with the local implementation of recommendations then supported by local specialist value for money auditors, the nascent OFLOG offered to “continue a programme of webinars to share best practice”.
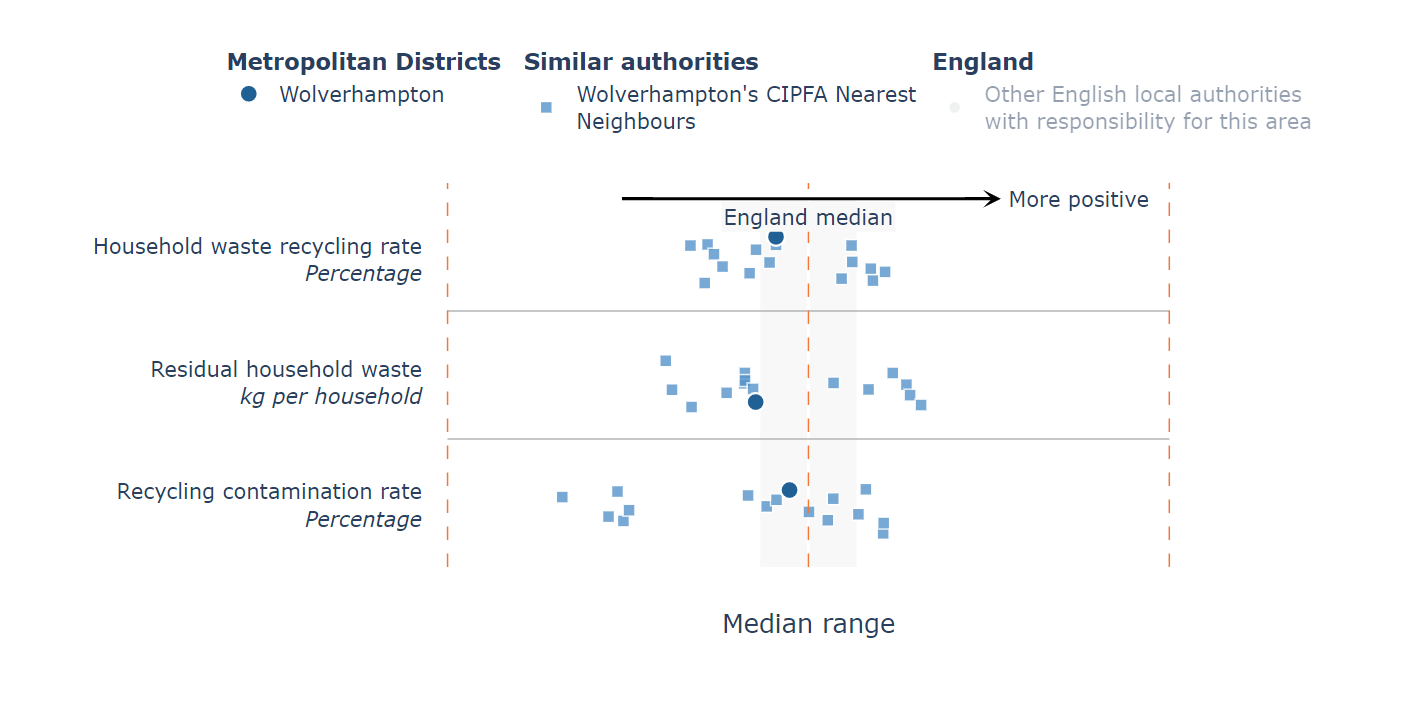
An early product of OFLOG, in July 2023, was its “Local Authority Data Explorer”, which now brings together PIs on waste management, planning, adult social care, roads, and corporate and financial issues. For each service, users can select three comparison councils to produce scatter charts like Figure 1, which compares my local council’s waste management with that of three other big cities. This led to some rather uninformed press commentary and a response from the LGA. One may also say this is perhaps not the most compelling presentation of data in the world, arguably significantly less clear or flexible than the LGA’s excellent Inform tool which has been freely available for several years and includes thousands of published metrics.
Caution should be applied to OFLOG’s position within a ministerial setting and the potential for politicians to be selective in how they use data for judging local authorities that are not of their political persuasion. Whilst some may argue that the former Audit Commission may have been too powerful, it did provide a greater degree of transparency and objectivity at interpreting performance data.
Figure 1: Waste management
As my colleague in Inlogov, Dr Philip Whiteman, has recently argued, the new government should ensure that OFLOG is independent of government with a remit to focus on:
Working with the sector to identify councils at risk of failure to ensure that support can be provided from within the sector, minimising the need for government intervention.
Collecting, analysing, and reporting data to enable individual councils, groups of councils and the sector nationally to make progress with shared priorities agreed with government.
Developing intelligence from on-going engagement with councils.
Supporting improvement in local services and councils’ contribution to national outcomes through researching, synthesising, and disseminating good practice.
Working with academic institutions such as Inlogov to incorporate key lessons from existing and future research.
We can be confident that local government performance overall is strong, and sector-led improvement has demonstrated our collective commitment to continuous improvement. But with so much of the new government’s ambitious “Missions” depending on highly effective local government, we need to take a fresh look at how OFLOG can be further developed to identify and propagate good practice across the sector.
Jason is Director of the Institute of Local Government Studies (INLOGOV) at the University of Birmingham and was employed by the Audit Commission from 1994 to 2004. This article was first published in the August 2024 LARIA Newsletter. Email [email protected]
INLOGOV’s new report, Equipping Local Government to Deliver National and Local Priorities, is available here.
Our two main political parties are locked in a strange debate about the next budget, on 6 March. The elephant in the room is the underfunding of local government.
In the nearly 14 years of Conservative government, the core spending power of local authorities has been cut by 27% in real terms.[1] The County Councils Network has “warned that its members are under extreme pressure, and that the authorities they represent are set to overspend by almost £650m this year due to spiralling costs, particularly in children’s social care and home to school transport, which was contributing to a £4b funding deficit for those authorities over the next three years”. In addition an increase in the National Living Wage is expected to costs these councils £230m next year.[2] This has happened at a time when the ability of councils to raise their council taxes has been held down, for 2024-5 to below 5% for all but a tiny number of councils.[3] One of its consequences has been the inability of the employers in local government and the NHS to negotiate pay settlements which reflect the rate of inflation, or anything near it.
My reading of the present position is that Gove on the one hand and Rachel Reeves on the other are playing chicken. Each are waiting for the other to move first. They both know that after the general election a new government will have to settle the long-standing pay disputes in the public sector, and that it is not possible, year after year, for the pay of staff employed by local government and the NHS to rise by less the rate of inflation. The consequences are visable: depressed morale, a haemorrhage of experienced staff, and dependence on immigration to employ new staff. Rachel hopes that the Conservatives will be forced to confront this before the election. Gove wants the Labour Party to commit to doing it, because as of now any settlement is unfunded.
My view is that the understanding of inflation both by the two main political parties and the Bank of England is naive, especially as it relates to government policy. The starting point should be that inflation affects the distribution of income. It is an intrinsically political process. Most large companies and the richest people have means through which they can compensate for any inflation. Those who do not have the power or muscle to do so pay the price. Thomas Piketty[4] showed that inflation was the main means by which the middle classes paid for much of the costs of two world wars.[5] In those inflations, and in the last significant inflation in the UK, which followed the OPEC hikes in oil prices in the 1970s, the trade unions were strong enough to ensure that wages rose at around the rate of inflation. This is no longer the case.
Yet the recent inflation has given the Government unprecedented increases in tax, which means that, if they so choose, they can afford wage increases. Most of this extra income arises from not raising the ceilings on higher rates of tax. Jeremy Hunt would like to use it to lower rates of income tax. The IMF (no less!) has told him that it is not appropriate to do so at this time.[6] The main reason, not always clearly stated, is that there are many unfunded challenges, but of these the public sector pay disputes (and perhaps the need for additional spending on defence, where difficulties in retention and recruitment are also partly a matter of pay settlements not keeping up with inflation) are top of the list.
Economists in the UK, the USA and other developed countries have had little to say in recent years about inflation. As if it is no longer a problem, which it probably isn’t if inflation stays at around 2%. But the present inflations, driven by wars, the climate crisis and the lockdowns, are another matter. Economic theory is little help. All the traditional theories have been shown to be false. It is not true that inflation and unemployment are opposites: we can have both together, so-called stagflation. Or that it can be controlled by limiting the supply of money, which is not possible when most of it is created by banks which lend far more than they hold in deposits. Or that it is either created by unexpected demands or by unexpected costs.
The British Government urgently needs to resolve the disputes about pay in the public sector, and to do so recognising that most local government employees are substantially worse off than they were before. The Labour spokesperson Angela Rayner has made the practical proposal of negotiating a three year settlement.[7] It cannot come soon enough.
Andrew Coulson is a nationally-recognised expert on scrutiny in local government and is particularly interested in governance by committee.
[3] A prescient academic law professor, writing as long ago as 1984, wrote “It seems to me that the provisions for rate-capping … are little removed from a proposal to replace elected councils by administrative units. For a very long time, local inhabitants have enjoyed the right to elect local representatives with the power to tax, and so to determine, within modest political limits, what level of services shall be provided in the locality. … I have no difficulty in saying of an Act to put a limit on the rates leviable by a local authority that it is politically unconstitutional”. John Griffiths, in the Preface to Half a Century of Municipal Decline 1935-1985, George Allen and Unwin, 1985, p.xii
[4] Thomas Piketty, Capital in the Twenty-First Century, Harvard University Press, 2014
[5] The point was also made by one of his critics, Joseph T Salano, “War and the Money Machine: Concealing the costs of War beneath the Veil of Inflation” in John V Denson (ed.) The Costs of War, Routledge, 2nd edn. 1999
The decision to create a new public body to inspect and regulate local authorities is a recognition that it was a major mistake, made by David Cameron soon after he became Prime Minister in 2010, to abolish the Audit Commission. At the time, many of us thought that the government would come to regret it. It is much easier to reform an existing body that to create a new one.
The Office of Local Government will be a Departmental body within Michael Gove’s Department of Levelling Up, Housing and Local Government’.[1] It will not, as was Audit Commission, be an independent public body. That leaves it wide open to the criticism that it is an extension of the process of central government bossing local government. The point has already been made in an influential report from the Institute of Government.[2]
OFLOG has already published what it calls draft “metrics” (or performance indicators) for some of the main services.[3] The Audit Commission began identifying performance indicators soon after it was created in 1983. It published its first comprehensive set of indicators for local government in 1992. In 2001 it instituted a process of Comprehensive Performance Assessments for every council, eventually based on more than 1,000 indicators. It used these, along with some qualitative assessments which attempted to assess a council’s ability to plan in advance and respond to crises, to give each council a rating on a scale of 1-5. In 2007 this was simplified, with just 214 indicators and a streamlined assessment where seven separate inspectorates worked together.[4]
This experience showed that there were fundamental problems. Performance indicators give providers very powerful incentives to change their behaviour. But they also give them powerful incentives to game the services, often by increasing spending on aspects that are measured and lowering it for those that are not.
Here are some high-profile examples:
The Police. Former senior police officer Rodger Patrick, in a pathbreaking PhD thesis at the University of Birmingham[5], showed how the West Midlands and other Police Forces gamed the statistics used to assess them: not recording many crimes, increasing clear-up rates by giving favours to criminals who confess (who might or might not have committed the crimes), moving police to parts of the city where the crimes committed can be dealt with relatively easily, and even creating what they claimed was evidence. Crimes were reclassified to reduce the apparent number of crimes in targeted areas.
Hospitals. Bevan and Hood used data from the National Audit Office to show that an unexpectedly large number of patients arriving in in accident and emergency departments were assessed just before they had waited four hours – thereby not contributing adversely to the per cent who waited longer. One way of doing this was not to record those waiting outside in ambulances or inside on trolleys. Another was to create Informal registers of people on long-term waiting lists, not putting many of them onto the official lists.[6]
Schools. OFSTED ranks schools as Outstanding, Good, Requires Improvement, and Inadequate. A poor score on any part of the assessment will prevent a school from being recorded as Outstanding. This became very public after a primary school headteacher took her own life when her school was downgraded for failing in its child protection arrangements while scoring highly in nearly all the other parts of its assessment. This case has led to increased awareness that a single judgement on a complex organisation such as a school can often be unfair or misleading when a school is strong in some aspects but less so in others.
These are not the only kind of problem. Another issue is that what is achievable will often depend on the history and geography of a place. Thus an area with many rail stations, or with very wide roads where bus lanes can be created, will find it easier to achieve targets for public transport. Or a city which is a regional centre will have a history of supporting local arts organisations, more so than a district which is not.
The third problem is that there is often duplication with other inspectorates: the Care Quality Commission, Ofsted, the Planning Inspectorate, Police and Crime Commissioners, and many others. Should OFLOT trust these, and not duplicate their work? Or should it follow the practice of the Audit Commission in its later years and work jointly with them, with associated extra costs and hassle?
We illustrate the issues with longer comments on one service, planning, where OFLOG has already produced detailed proposals.[7] I wrote about this in 2007, and the proposals I discussed then are almost identical to those proposed now.[8] These will judge the effectiveness of planning in an area by the number of planning applications dealt within a target number of days, and the percent of applications overturned after appeals. This does not recognise that the most important work is done well before an application is formally submitted, when an applicant or agent starts talking to officials in the planning department. This may well throw up problems with transport or access; lack of proposals for green space, community facilities or shops; environmental issues about trees or wildlife; and disagreements about densities. The Council will want as many units as possible on a site, and for an application to meet its requirements for social and affordable housing. Moreover, drawings are often inaccurate, computerised images misleading, surveys loaded to favour an application, and designs poor. Good quality advice can make a big difference. But if an application is submitted before these matters have been properly researched, or do not meet the council’s prescriptions (especially for affordable housing), it has to decide whether or not to take it to its committee recommending rejection, or to wait for a more comprehensive submission to arrive. The easiest way to meet these targets is for councillors to approve every planning application uncritically.[9] Developers frequently try to renegotiate targets for social and affordable housing units, on the basis that they cannot afford them. But with only very limited other funding for this type of housing, they are essential almost everywhere. This kind of stand-off will no doubt continue unless and until land values decline to the point where developers can both meet the targets and make money.
In short, the OFLOG draft targets for the planning function are a missed opportunity. What is needed is powers to refuse planning applications that do not include relevant evidence or meet the prescriptions set out in a council’s local plan without wasting the time of the Planning Committee. And targets which explicitly recognise the value of design and quality, and the need for social facilities and open space.
These issues are not confined to planning. At a time of austerity which especially affects the funding of local government, there will inevitably be many situations where councils are struggling to deliver services of the quality that they would like. In such situations, inspectors do not contribute much by pointing this out. Rather they need to act as advisors, or expert external friends, who assist councils making the most of what they have.
Andrew Coulson was an INLOGOV staff member for 25 years. For 14 of those years he was also a Birmingham City Councillor where for a time he was a member of the Development Control Committee as well as the Cabinet Member for Regeneration.
[1] Department for Levelling Up, Housing, and Communities and Office for Local Government Understanding and supporting local government performance. Policy Paper, July 2023
[4] Andrew Coulson “Targets and Terror: Government by Performance Indicators. Local Government Studies Vol.35, No.2 pp.271-81, 2009
[5] For a summary, see Rodger Patrick,“A web of deceit: Police Crime Statistics for England and Wales”, in John Eterno, Arvind Verma and Eli Silverman (eds) How Countries Count Crime: An Exercise in Police Discretion Taylor and Francis, 2022, pp.170-219
[6] Bevan, G and Hood, C “What’s Measured in What Matters: Targets and Gaming in the English Public Health Care System”. Public Administration Vol.84, No.3, pp.517-38
[7] Office for Local Government Next steps for OFLOG and draft metrics, October 2023, pp.5-7
[8] “Don’t Forget the Politics in Planning”. Local Economy Vol.22 No.3, pp.223-6
[9] “Targets and Terror: Government by Performance Indicators.” Local Government Studies Vol.35 No.2, 2009, p.279
Relations between first and second cities are often strained, especially when those who live in the Second City elect leaders from a political party that is not running the national government – as has been the case with Birmingham for much of its life.
After the Second World War, Birmingham was prosperous. It had avoided most of the bombing that destroyed the centre of Coventry, and its factories had produced aircraft, lorries, and other vehicles and equipment for the military and were now available to meet the post-war demand for cars and lorries. Wages for semi-skilled labour were some of the highest in the country. There were shortages of labour, and to meet them employers welcomed bus drivers, conductors and nurses. These were followed in the 1970s and 1980s by workers mainly from Pakistan and Kashmir.
From the perspective of the London government, Birmingham did not need more employment, so companies who wished to invest in the motor industry were directed to Liverpool and elsewhere. But academic commentators, and the more thoughtful employers, could see that all was not well. Britain was becoming increasingly dependent on service industries, which were far from strong in the Midlands. In that context, in the mid-1970s, Birmingham Council proposed to build a National Exhibition Centre, on land near the airport. It would be owned by a company which was a partnership with Birmingham Chamber of Commerce. The government wanted it in London; the council carried on regardless, and eventually the London government allowed it to do so.
Its structure was innovative – the company had just two shares, one owned by the city council, the other by the chamber. Each could nominate four directors. The chair would always be one of the chamber nominees – for a long time the leading industrialist Sir Adrian Cadbury. But if voting on the board was tied, the chair did not have a casting vote, and what was proposed would not go ahead. The company, underwritten by the council, borrowed money and built the NEC.
A few years later, in 1987, the NEC company started building the International Convention Centre and Symphony Hall, on land off Broad Street. This was to make Birmingham a centre for conferences and business meetings. The decline in manufacturing and rising unemployment was by then so evident that Birmingham was granted Assisted Area Status by the European Union, so a fraction of the cost was met from Europe. The London government was not involved.
The ICC became a preferred location for large gatherings of professional bodies, such as the British Small Animal Veterinary Association, which grew till it hosted more than 8,000 delegates. It met in Birmingham every year for more than 25 years. A boom in the construction of hotels met the demand for accommodation for this kind of event. Also of offices, many taken by national or international companies. No longer is Birmingham lagging in its provision of services. On the contrary it is a leader – almost entirely because of these initiatives. Symphony Hall was built to meet the specification of Simon Rattle, then a very young but highly promising conductor of the City of Birmingham Symphony Orchestra. It was part of a city-council strategy to support the arts, of which another strand was the attraction of what became the Birmingham Royal Ballet to the Hippodrome theatre – with its charismatic directors, Peter Wright, David Bintley and now the Cuban star Carlos Acosta. Another initiative required investors in large buildings to put a small extra amount aside for public art.
The arrival of a national Conservative government in 2010 meant that the council started losing the extra grant it had long enjoyed to meet its high levels of deprivation, and put it under huge financial pressure. Whole levels of staffing in departments of the council were removed. Many senior officers did not stay long. Some posts were not filled. Others are filled by ‘interim’ staff, who are supplied by agencies, do not expect to stay in the city and are very unlikely to live in it.
The refuse collection service was traditionally headed by an assistant director who had worked in the service for many years. For a period before the 2017 strike, this post was not filled, and the service was for a time run by the director of leisure. The strike was about reducing the number of operatives on each vehicle when wheelie bins were introduced. It was resolved by giving the workers improved pay.
It appears that it was only later that the implications of this for ‘single status’ were recognised, meaning that other categories of workers – in particular in social care – could claim equal pay for work assessed as equivalent. To meet the huge resulting costs, the city sold the NEC company for £300m. It was resold for £800 million three years later – a warning to the current commissioners not to sell this kind of asset on the cheap. Since then, the bin workers have managed to complete their shifts in less time than expected – partly assisted by some residents not putting their bins out every week – and been permitted to sign off early when their round was completed. Again, it has only recently been realised that this opens the city to another round of ‘single status’ claims. Hence the near bankruptcy, Section 114 Notice, and appointment, by Michael Gove in London, of commissioners.
To resolve challenges such as this, when Birmingham is facing extreme pressures on all its services, will not be easy for the commissioners.
The worst thing they could do would be to split Birmingham into perhaps three smaller councils. This would increase the overhead costs – three directors of each service instead of one, three separate offices – and lose major economies of scale. It would also threaten the leadership and finance which is part of being the Second City – in the arts, in the representative institutions of local government, and in creating and implementing an economic strategy which responds to the local opportunities and needs which are most clear to people living in the city.
Andrew Coulson is a retired lecturer from INLOGOV and a former Birmingham City Councillor. A longer version of this article was published in The Birmingham Post. Andrew writes in a personal capacity.
Maybe you love it, maybe you hate it, maybe you are somewhere in between. Either way you know that remote working is here to stay. Should we be happy with how it’s going though? Are public services adapting or struggling with this new normal?
A lasting legacy of the pandemic, the expansion of remote working is definitely seen a good thing by many public servants. Less travelling, a chance to keep an eye on things at home and a chance to stick the washing on. You can have your work space exactly how you want and, when so many public services are looking to save money on costly office accommodation, it helps with that as well.
Of course, it doesn’t work for everyone. Unwanted interruptions, not having a good space to work in and missing those ‘water cooler’ conversations are all negatives. Also, isolation, professional and social, can take its toll and affect mental health. It’s no fun taking a distressing call in your own home with no-one around to talk to about it afterwards.
Three years on from the first shock of the pandemic, a more complex picture of remote working is starting to emerge – something that we are picking up as part of refreshing the 21st Century Public Servant research 10 years on (link in the comments).
For example, is there something concerning about the way that remote working can divide teams? After all, when Joe is working at home the rest of us are left to answer the office phones or respond to the people turning up the front desk – and Jane is worried that Joe might not be really working at all. He certainly seems invisible.
There are also worries about people who joined their teams during lockdowns and formed their relationships with co-workers over Zoom. How might starting a job in ‘virtual limbo’ affect people when they finally start to meet their team in person?
We’ve also come across the idea that long term remote workers form stronger relationships with virtual co-workers and find it easier to distance themselves from work relationships they see as negative – perhaps withdrawing from their teams in a way that office-based staff might not.
And what about citizens? On the one hand public servants can be more accessible and might have more time due to less travel but is the quality of their interactions affected? When public servants are being asked to be more relational in their work can this be achieved in the same way through Teams or Zoom?
The challenge for public servants, it seems, is to adapt to remote working, or perhaps more accurately, to hybrid workplaces. To maintain the benefits of remote working while staying connected to co-workers and to the communities they serve.
We think it’s an intriguing topic of research and we are looking to learn more…
Dr Dave McKenna is an independent consultant and researcher who helps councils and other public bodies with training, research and improvement work. He is part of the research team currently updating our 21st Century Public Servant framework.
With under 700 days to the next UK general election, political parties are busy developing their manifesto documents. In February, Labour leader Keir Starmer made a major speech laying out his “five missions for a better Britain”. How do these five missions relate to local government? And is the turn to “mission driven” government likely to work?
The five missions vary in their level of specificity and challenge. Securing “the highest sustained growth in the G7, with good jobs and productivity growth in every part of the country…” is a little vague but likely to be difficult, especially given we are currently ranked 6 out of 7 in terms of output per worker. Mission #2, “make Britain a clean energy superpower”, accelerating the move to zero-carbon electricity from 2035 to 2030, is specific but very challenging. Mission #3, reform of health and social care and reducing health inequalities, will require a re-focus from secondary (hospital) care to social care and addressing the social determinants of health. Mission #4 is about community safety, and likely to involve more community policing. Finally, mission #5 is to “break down the barriers to opportunity at every stage” through reform to the childcare and education systems.
Local government potentially has important roles in each of the five missions. Local education, skills and economic development functions will be critical to improving productivity. On energy, Net Zero requires at least a doubling of electricity generation by 2050, from decarbonised sources. Decarbonisation strategies need to be place-based, taking account of the geography, building types, energy infrastructure, energy demand, resources and urban growth plans. We’ve recently argued here for the key roles of councils in this area.
Turning to health and care services, local government clearly has leading roles – including ensuring place-based planning to address the social and behavioural causes of health inequalities. Analysis by the Liverpool and Lancaster Universities Collaboration for Public Health Research in 2021 concluded: “investment across the whole of local government is needed to level up health including investment in housing, children’s, leisure, cultural, environmental, and planning services”. Similarly community safety, child care and education are areas where local government could be enabled to have much greater positive impact.
Perhaps as important as the specific “missions” is the approach to governing which the party is proposing. Labour’s document characterises this as a move from top-down, target-led, short-term, siloed approaches, to government which is more “agile, empowering and catalytic”, working across the public and private sectors, and civil society. This, it argues, requires organising government around a shared vision, focusing on real world outcomes, concentrating on ends with flexibility and innovation concerning means, devolving decision making from Westminster, increasing accountability including central and local data transparency, and adopting long-term preventative approaches including greater financial certainty for local areas.
In some ways the idea of mission-driven government echoes the 1990s thinking of Ted Gaebler and David Osborne’s book “reinventing government”, which argued for a more entrepreneurial approach to the delivery of government. Their work pointed to entrepreneurial companies setting overall missions and goals, and then leaving managers to figure out how best to deliver these – for example, by providing an overall budget for a service rather than detailed line-by-line budgets which disappear if not spent by year end. The focus on managers rather than considering the perspective of politicians is one of the problems identified in subsequent evaluations of the reinventing government model, together with difficulties in sustaining the approach.
Mission-driven policies addressing ‘grand challenges’ of society are increasingly common, for example in the UN Sustainable Development Goals and various EU policies. Mazzucato et al recently argued that addressing such challenges requires strategic thinking about: the desired direction of travel, the structure and capacity of public sector organisations, the way in which policy is assessed, and the incentive structure for the private, public (and I would add community) sectors. Labour’s paper makes a start (albeit at a very high level) on thinking through these areas. The litmus test, though, will be in developing the detail and how far this engages with local areas.
Over the next few months, we will be contributing to the debate on the upcoming party manifestos with some research-informed thoughts on a variety of local government related policy areas. If you would like to be involved in developing these, please get in touch.
Jason Lowther is the Director of INLOGOV. His research focuses on public service reform and the use of “evidence” by public agencies. Previously he worked with West Midlands Combined Authority, led Birmingham City Council’s corporate strategy function, worked for the Audit Commission as national value for money lead, for HSBC in credit and risk management, and for the Metropolitan Police as an internal management consultant. He tweets as @jasonlowther