We know our GPs are busy; and indeed, during my visits, I have seen how hard they work — my own doctor is amazing. But I also hear, too frequently, from our residents of their struggles to get an appointment, to use online systems or to see a GP in person.
As a Brent councillor, I chair two health committees — one in Brent, and the other covering the 8 NW London boroughs — and I am proud of our NHS, in this 75th anniversary year, particularly our primary care service.
So, a few days ago, I was pleased to welcome GPs from across NW London to Brent and to hear about some of the changes our local NHS is implementing to help us all get the very best from our GP surgeries.
A new campaign from NHS NW London, We Are General Practice, explains the different people who are now working in our GP surgeries. I have met with GPs from across NW London, and they have spoken about how sometimes our residents do not actually need to see a GP — they can see a specialist like, say, a diabetes nurse, a pharmacist, or a physiotherapist. In many places, these people are now working side by side with the GP in the same building which, of course, is fantastic for patients.
Not only does this ease the pressure on our GPs but it means that, as a patient, you will be seen by the best possible person in a timely manner.
Also, what is special about this campaign is how it has used input from our residents. We often hear the phrase “co-produced”. Well, this is, perhaps, the best possible example of that phrase. The teams in NW London, who are always out and about across the boroughs listening to residents, have taken on board what they have heard and used it to shape, not just the campaign, but the improvements we are beginning to see across our general practices.
We, in local government, of course, have a part to play. Not only are we more formally in partnership with the NHS locally now but we are all here to support the same people. The NHS call them patients, we call them residents. And we can all support people navigating their way through services and help with the sign posting and support.
So, my thanks to all those residents who shared their experiences and views on how our health services can improve.
Our GPs, and their teams, do such a lot to keep us all well and I am pleased to see this campaign shine a light on all the people that make up a general practice team.
Cllr Ketan Sheth chairs the North West London Join Health Scrutiny Committee
The earthquakes that took place in Maraş province of Turkey on February 6, together with the terrible destruction they caused, also led to the questioning of state institutions and capacity. An important dimension of the subject is the relationship between central and local governments in the country. These earthquakes and what happened afterwards have been instrumental in questioning the overcentralized structure of the state in Turkey[i]. Discussions centered on why the earthquakes were so devastating[ii] as well as the inadequacies in the post-earthquake response[iii].
In Turkey, the authority to issue city planning and zoning permits belongs to the central administration. The authority to carry out urban transformation processes in existing settlements also rests with the Ministry of Environment, Urbanization and Climate Change, which is the relevant ministry of the central government. Therefore, the possibilities of municipalities to make cities earthquake resistant are very limited. The authorities of municipalities, such as controlling and licensing the buildings against earthquakes, are not used effectively enough.
Turkish people have witnessed that the excessively centralized structure also hindered the post-earthquake rescue efforts. It was not possible for local actors to take the initiative and act. The lack of timely mobilization of local capacity increased the loss of life. It is very important that not only local governments, but also civil society mobilize in such crises. However, there was a process in which non-governmental organizations and volunteers carrying out aid campaigns were also targeted[iv]. In a televised speech to the nation, President Erdoğan complained about critical news and declared that he planned to hold critical voices to account. Later, access to Twitter was throttled while rescue operations were still underway. The government claimed that it did so to prevent “disinformation”. Some government actors and their supporters also raised concerns about the extent to which public support and fund-raising has been directed at civil society organizations like Ahbap, rather than the government’s own relief organization, AFAD.
In fact, we have witnessed such challenges to local actors in the face of complex and multiple crises by the central government before. For example, during the coronavirus pandemic, the efforts of the Istanbul Metropolitan Municipality to collect aid were stopped and the donations amounting to 6.2 million liras collected in the bank accounts were confiscated and transferred to the central government bodies[v]. The 3.5 million lira aid collected by the Ankara Metropolitan Municipality was blocked. The solidarity campaigns of municipalities were evaluated by President Erdogan as “the logic of being a state within a state”[vi]. Determining the policies and practices related to the pandemic from a single center instead of being shaped according to local conditions increased the negative effects of the pandemic on the society.
Municipalities were also left alone in the refugee issue, one of the deepest crises Turkey has experienced recently. Even municipalities with a refugee population of up to a quarter of their own population did not receive a penny of additional support from the central budget[vii]. Moreover, municipalities do not know what to do about refugees, as there is no clear legislation and coherent policy in this area. While the discourse and policy towards refugees shifts from hospitality and religious solidarity to ‘voluntary’ return, municipalities are forced to cope with this uncertainty[viii]. Despite this, they develop and implement creative and entrepreneurial projects in cooperation with civil society to meet the needs of refugees and integrate them into society[ix].
The European Charter of Local Self-Government[x], signed by Turkey in 1992, obliges the parties to implement the basic rules that guarantee the political, administrative and financial independence of local governments. Despite this Charter, which provides for the recognition of the principle of local self-government in domestic legislation and, if possible, in the constitution, trustees appointed from the center serve instead of those elected[xi]. At the local elections on March 31, 2019, the HDP (Peoples Democratic Party) won 65 municipalities in the Kurdish-majority provinces. While six of the elected mayors were not given their certificates of election, trustees were appointed by the central government to 3 metropolitan, 5 provincial, 45 district and 12 town municipalities. While the municipalities are under such tutelage in regions where Kurdish voters are concentrated, a politically motivated judicial process hangs like the sword of Damocles over the head of Ekrem İmamoğlu, Istanbul Metropolitan Municipality’s elected mayor[xii].
Earthquake is one of the realities of Turkey. However, the strict centralist structure and the authoritarian regime, which further increases its negative impact, prevent local initiatives, resilience and solidarity not only in earthquakes but also in all kinds of crises that arise today. Complex crises such as pandemics, mass migration and climate change that we have faced in recent years and will face in the future are far from being problems that a single actor can deal with at a single level. It is not possible to deal with these crises without vertical cooperation between local, national and international levels of government and horizontal cooperation networks between state and non-state actors such as civil society organizations.
Although we can see the damages of over-centralized administration most clearly in times of crisis, the cost of not having resilient and participatory local government that meets local demands is much greater than we think. Local governments cannot be ‘local’ enough because they are financially dependent on the center and because of the arbitrary and partisan practices of the central government. If this earthquake is to be a start, taking big steps to strengthen local democracy should also be a part of it.
Rabia Karakaya Polat is a professor of political science at the Department of International Relations at Işık University (Istanbul). She recently completed a British Academy-funded joint research project, with Prof. Vivien Lowndes, analysing local refugee policies in Turkey. She published numerous articles in journals such as Security Dialogue, South European Society and Politics, Citizenship Studies, Parliamentary Affairs, Government Information Quarterly, Local Government Studies and Journal of Refugee Studies. Currently, she is working on refugee integration policies at the local level.
[i] Cemal Burak Tansel (2020) Reproducing Authoritarian Neoliberalism in Turkey: Urban Governance and State Restructuring in the Shadow of Executive Centralization, Authoritarian Neoliberalism, Routledge, 88-103
[viii] Vivien Lowndes & Rabia Karakaya Polat (2020) How do local actors interpret, enact and contest policy? An analysis of local government responses to meeting the needs of Syrian refugees in Turkey, Local Government Studies, 48:3, 546-569
[ix] Rabia Karakaya Polat & Vivien Lowndes (2022). How does multi-level governance create capacity to address refugee needs, and with what limitations? an analysis of municipal responses to Syrian refugees in Istanbul. Journal of Refugee Studies, 35(1), 51-73
If local councils and the NHS do not work together as trusted equal partners, our residents are the ones that lose out.
In Brent, our local communities were among those most affected by the first and second waves of the Covid-19 pandemic, with the local hospital, Northwick Park, making the national headlines having been caught in the eye of the storm, which acutely demonstrated the terrible impact of health inequalities on real lives.
We are, of course, particularly reliant on our NHS partners to provide emergency services, planned elective care, and a full and complex mix of outpatient and specialist services, including mental health and community services.
Likewise, NHS staff are reliant on local councils (and other local partners) playing their part in delivering a seamless patient pathway, that can go from a first GP visit right through to a tailored social care package.
Delivering high quality, equitable health services take detailed planning and a solid grasp on the needs of local communities.
In Brent, we have seen increasing levels of partnership working with the local NHS trust. Collaboration is made easier because London North West University Healthcare NHS Trust (LNWH) shows a refreshingly genuine commitment to gaining a deep appreciation of the views, concerns, and perspectives of our local populations. This is reflected in the development of the trust’s new five-year strategy.
In addition to undertaking vast analysis of public health, demographic and other data relating to our communities, LNWH sought engagement right from the start. The trust co-created a strategy with the help of almost 900 local community members and 40 representatives from local authority and partner organisations. Over 2,300 staff also contributed, many of who live locally and reflect the diverse population of our local communities and are frontline NHS staff who know all too well the importance of good partnership working.
I hosted one of the open forums for the trust where the local residents had an opportunity to say what they felt should be the trust’s priorities. Working in partnership with local communities and improving the quality of care came out as key themes.
This is not surprising. In Brent, our communities experience significant health inequalities when compared with regional and national levels. Local councils like Brent can only provide so much support to address these issues, so we must work with NHS partners to combat health inequalities right across our health and social care system. Indeed, we are now seeing an increased trust present at place-based and neighbourhood meetings.
One of the biggest challenges facing LNWH is the level of emergency activity. As a local council, we must work collaboratively to address systemic issues like this that the trust cannot resolve alone. Indeed, the emergency pathway is a key touchpoint for the most deprived people in Brent and partnership working presents us with a real opportunity to connect them earlier with more appropriate support in the community.
The trust’s discharge processes are perhaps the most reliant on partnership working — the NHS isn’t just its hospitals. It’s vital that we work collaboratively across organisations — the rest of the local NHS like GPs, district nursing, mental health and social care — to help the trust improve the flow of patients through its hospitals.
LNWH has called its new five-year strategy ‘Our Way Forward’. It sets out a welcome commitment to local authorities, communities, and people. We must take joint responsibility for Our Way Forward, because by working together we will forge a far better health outcomes for our residents than we can alone.
Cllr Ketan Sheth is Chair of North West London Join Health Scrutiny Committee
With under 700 days to the next UK general election, political parties are busy developing their manifesto documents. In February, Labour leader Keir Starmer made a major speech laying out his “five missions for a better Britain”. How do these five missions relate to local government? And is the turn to “mission driven” government likely to work?
The five missions vary in their level of specificity and challenge. Securing “the highest sustained growth in the G7, with good jobs and productivity growth in every part of the country…” is a little vague but likely to be difficult, especially given we are currently ranked 6 out of 7 in terms of output per worker. Mission #2, “make Britain a clean energy superpower”, accelerating the move to zero-carbon electricity from 2035 to 2030, is specific but very challenging. Mission #3, reform of health and social care and reducing health inequalities, will require a re-focus from secondary (hospital) care to social care and addressing the social determinants of health. Mission #4 is about community safety, and likely to involve more community policing. Finally, mission #5 is to “break down the barriers to opportunity at every stage” through reform to the childcare and education systems.
Local government potentially has important roles in each of the five missions. Local education, skills and economic development functions will be critical to improving productivity. On energy, Net Zero requires at least a doubling of electricity generation by 2050, from decarbonised sources. Decarbonisation strategies need to be place-based, taking account of the geography, building types, energy infrastructure, energy demand, resources and urban growth plans. We’ve recently argued here for the key roles of councils in this area.
Turning to health and care services, local government clearly has leading roles – including ensuring place-based planning to address the social and behavioural causes of health inequalities. Analysis by the Liverpool and Lancaster Universities Collaboration for Public Health Research in 2021 concluded: “investment across the whole of local government is needed to level up health including investment in housing, children’s, leisure, cultural, environmental, and planning services”. Similarly community safety, child care and education are areas where local government could be enabled to have much greater positive impact.
Perhaps as important as the specific “missions” is the approach to governing which the party is proposing. Labour’s document characterises this as a move from top-down, target-led, short-term, siloed approaches, to government which is more “agile, empowering and catalytic”, working across the public and private sectors, and civil society. This, it argues, requires organising government around a shared vision, focusing on real world outcomes, concentrating on ends with flexibility and innovation concerning means, devolving decision making from Westminster, increasing accountability including central and local data transparency, and adopting long-term preventative approaches including greater financial certainty for local areas.
In some ways the idea of mission-driven government echoes the 1990s thinking of Ted Gaebler and David Osborne’s book “reinventing government”, which argued for a more entrepreneurial approach to the delivery of government. Their work pointed to entrepreneurial companies setting overall missions and goals, and then leaving managers to figure out how best to deliver these – for example, by providing an overall budget for a service rather than detailed line-by-line budgets which disappear if not spent by year end. The focus on managers rather than considering the perspective of politicians is one of the problems identified in subsequent evaluations of the reinventing government model, together with difficulties in sustaining the approach.
Mission-driven policies addressing ‘grand challenges’ of society are increasingly common, for example in the UN Sustainable Development Goals and various EU policies. Mazzucato et al recently argued that addressing such challenges requires strategic thinking about: the desired direction of travel, the structure and capacity of public sector organisations, the way in which policy is assessed, and the incentive structure for the private, public (and I would add community) sectors. Labour’s paper makes a start (albeit at a very high level) on thinking through these areas. The litmus test, though, will be in developing the detail and how far this engages with local areas.
Over the next few months, we will be contributing to the debate on the upcoming party manifestos with some research-informed thoughts on a variety of local government related policy areas. If you would like to be involved in developing these, please get in touch.
Jason Lowther is the Director of INLOGOV. His research focuses on public service reform and the use of “evidence” by public agencies. Previously he worked with West Midlands Combined Authority, led Birmingham City Council’s corporate strategy function, worked for the Audit Commission as national value for money lead, for HSBC in credit and risk management, and for the Metropolitan Police as an internal management consultant. He tweets as @jasonlowther
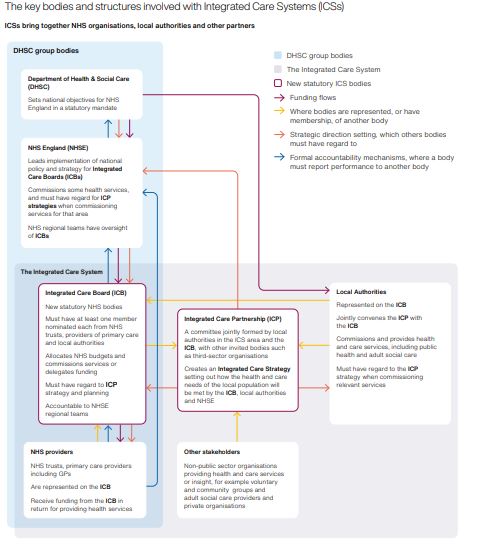
As the government once again kicks down the road decisions on vital reforms and funding for social care, local areas are establishing the Integrated Care Boards which will lead the new Integrated Care Systems (ICS), bringing together the NHS, local government and partners to plan and deliver integrated services to improve the health of the local population. Building on the progress made since many public health responsibilities transferred back to local government in 2013, this is a great opportunity to address the determinants of health and issues around health inequality. Might ICSs at last lead to an effective local voice in our over-centralised, top-down healthcare system?
Each ICS is supposed to plan at three levels: the neighbourhood (an area of around 40,000 people), the ‘place’ (often a LA area), and the (ICS) system (covering around 2 million people). Working at the neighbourhood level is likely to be somewhat informal, often using a social prescribing approach and developing multi-disciplinary teams including third sector partners. The approach to ‘place’ looks set to vary between areas, with some ICSs devolving significant responsibility (and funding) whilst others centralise these at ‘system’ level. Meanwhile at ‘ICS system’ level, Integrated Care Partnerships (joint LA and health committees) will develop an Integrated Care Strategy to meet the assessed health and social care needs of their population identified in the Joint Strategic Needs Assessments and Wellbeing Strategies prepared by local Health and Wellbeing Boards.
Beyond the formal planning process, the success of local ICSs will partly depend on the quality of local collaborative (managerial and political) leadership – across statutory partners and with the third sector. It will be a tough job to balance the priorities of the national health service and issues of local places, but many local authorities will be able to offer helpful experience , for example from moves to more networked governance approaches.
The National Audit Office recognises the potential but appears dubious on current prospects. Last month it published a review, Introducing Integrated Care Systems: joining up local services to improve health outcomes, finding:
“NHSE has a detailed regime to monitor performance against core NHS objectives but … it is less clear who will monitor the overall performance of local systems, and particularly how well partners are working together and what difference this new model makes…“
The report notes that, whilst government is asking ICSs to set out local priorities and make progress against them, there is no protected funding and few mechanisms to ensure this happens. This leads, as the NAO politely puts it, to “a risk that national priorities, and the rigorous oversight mechanisms in place to ensure they are delivered, crowd out attempts at progress on local issues”. The report also identifies five “high risk” elements of effective integration: clarity of objectives, resourcing, governance and accountability (such as how ICSs will function alongside existing local government Health and Wellbeing Boards and how accountability differences between NHS and local authority bodies will be resolved), and the capacity to balance priorities other than national NHS targets. These urgently need to be addressed if ICSs are to begin to meet their potential.
At one of Inlogov’s “Brown Bag Lunch” discussions earlier this month we agreed on the importance of issues around how ICSs develop, particularly in terms of developing effective system leadership and planning, collaborating with community organisations, and links to wider devolution processes. I’d be interested to hear about experiences in local areas as these develop.
Jason Lowther is the Director of INLOGOV. His research focuses on public service reform and the use of “evidence” by public agencies. Previously he worked with West Midlands Combined Authority, led Birmingham City Council’s corporate strategy function, worked for the Audit Commission as national value for money lead, for HSBC in credit and risk management, and for the Metropolitan Police as an internal management consultant. He tweets as @jasonlowther
Black History Month creates a moment when we can step back and reflect together, as well as individually, on the immense contribution of Black, Asian and minority ethnic communities whose rich history, culture, and experiences, have shaped Brent and beyond.
The NW London Joint Health Scrutiny Committee comprises 8 NW London boroughs. As Chair, I know we simply could not function without the dedication, the skills, and above all, the compassion that thousands of people from our diverse communities contribute to the NHS, day in and day out.
The difference this makes to all our lives, is immeasurable. Black History Month affords us an opportunity to acknowledge and thank them for the important work they do: their continuing contribution to the care, the culture, the shaping, and well-being of Brent.
The colour of someone’s skin should not determine how they are perceived, considered, and treated – positively or negatively – but the impact of the pandemic has highlighted many disturbing features of inequality in our communities. Many of these problems are not new. They have existed for far too long.
Black, Asian and minority ethnic communities are more likely to be affected by life-changing diseases like diabetes, prostate cancer, and sickle cell than people from other backgrounds. Living in less-affluent areas, they are more greatly affected by poor housing as well as poor air quality from the busy urban roads that run through their neighbourhoods. There is a big gap in life expectancy between richer and poorer areas irrespective of race, but these communities are disproportionately affected.
To tackle these inequalities, the North West London Integrated Care System is launching a joint initiative between the local NHS and NW London boroughs, which will seek to build real understanding of what matters to our residents, how we can work with them to remove barriers to health equality to deliver healthier neighbourhoods and better outcomes.
This initiative is the first tangible benefit I have seen emerge from the new Integrated Care System, which has health services and local authorities coming together to address many of the challenges that impact our well-being. That is, health and care services, employment, education, housing, and the environment we live in.
We might perhaps reflect for a moment on the work of the great poet, James Berry OBE, who never avoided the difficult issues of injustice in history, or in the present, but always sought for mutual understanding. His poem, “Benediction,” stresses the need for us truly to hear one another, and truly to see, and through so doing, to understand. He said:
Thanks to the ear that someone may hear
Thanks to seeing
that someone may see
Thanks to feeling
that someone may feel
Thanks to touch
that one may be touched…
Black History Month is a reminder to us to truly hear and see one another, to celebrate our heroes and tell the stories that, for so long, have been hidden or forgotten. It is also a reminder that the evils of the past have resonance today, reflected in the impact of poverty and institutional racism that many in our communities experience as part of their daily lives. Ultimately, it is an opportunity to continue to learn, understand and come together to pull down these barriers and build healthier and fairer neighbourhoods.
Cllr Ketan Sheth is Chair of Brent Council’s Community and Wellbeing Scrutiny Committee